
A chair, asking and listening to the patient: the key element to focus a diagnosis
A chair, asking and listening to the patient: the key element to focus a diagnosis
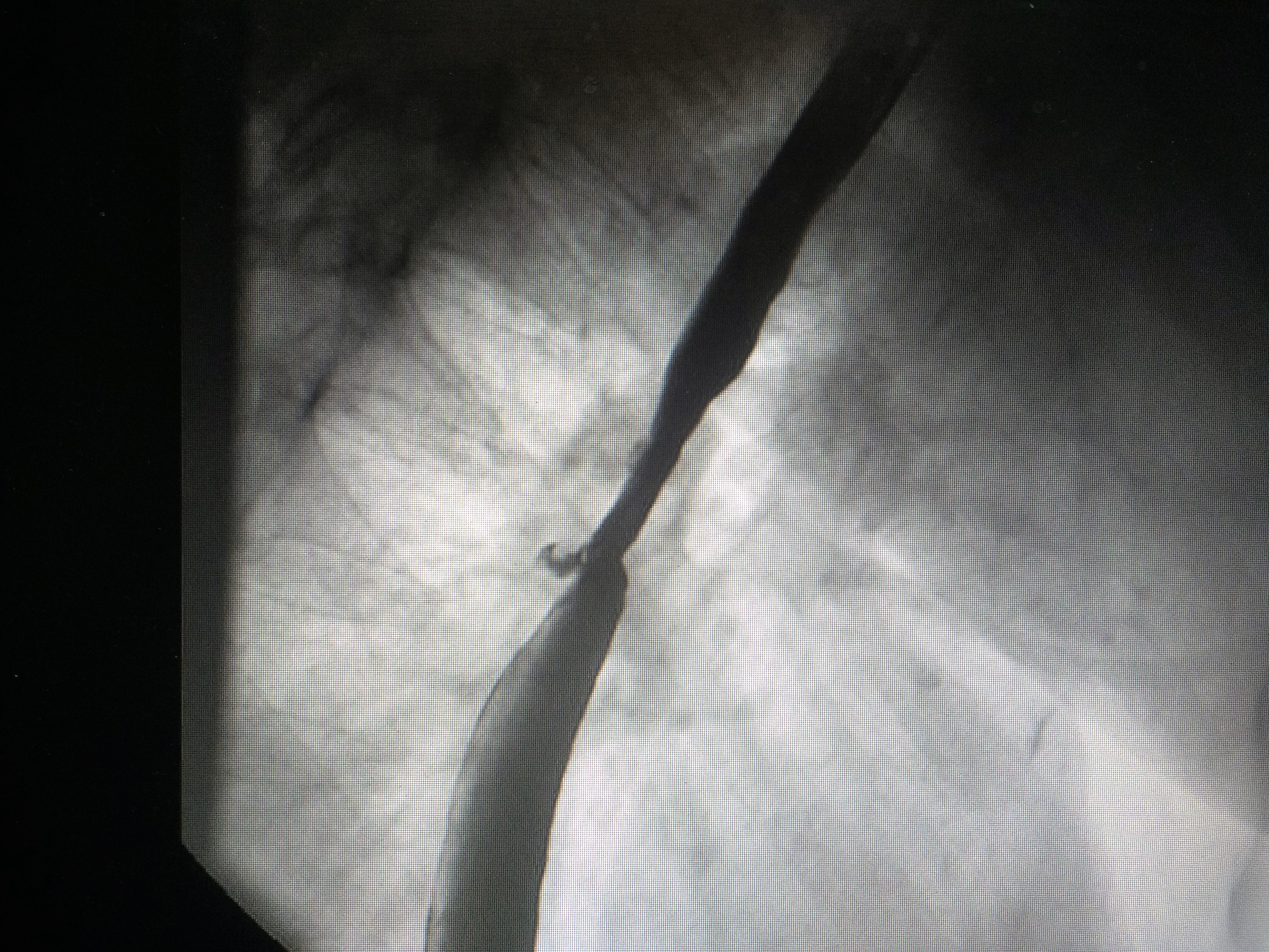
Patient with a previous diagnosis of non-small cell lung cancer. He had a prosthesis placed on his esophagus to correct a tracheal and bronchial fistula. With this device he could eat and swallowed normally.
During a 6-month period of treatment with immunotherapy , the patient went to the clinic on several occasions with shortness of breath, cough and little expectoration, and sometimes with fever, suggesting a respiratory infection to the doctors most of the time.
But the symptoms persisted
The patient stayed in the hospital again with a deterioration of the respiratory function, together with fever and mild cough and expectoration. No bacteria were isolated in the blood and sputum culture. The CT scan showed no major changes. More steroids and antibiotics were added to the treatment, but without improving.
Clinical reasoning
When a patient with a tumor is not improving with a proper treatment for a respiratory infection, the physician should follow a “logical” path to achieve a good outcome. First, we have to know the situation of the tumor, comparing the actual test with previous. Secondly, we have to discharge a possible adverse event associated with a new treatment, and the third recommendation is to pay attention to the context of a particular patient, his or her specific situations what can give the clue to reach a diagnosis. But, to get a satisfactory outcome, we need time to listen to the patient, asking questions that can help to solve the clinical picture.
Solution to the problem
The dyspnea increases when after drinking milk and liquids. It was clear that the fistula was not covered by the prosthesis.



