
Why Can Right Heart Failure be Mistaken for Sepsis? A Clinical Reasoning Exercise

Objective
In this article, we want to show the importance of knowledge of Anatomy and Pathophysiology in clinical reasoning, presenting a real clinical situation, in which it is necessary to differentiate between entities that may share symptoms and analytical data, but have a different therapeutic approach. In addition, the development of new drugs in Medical Oncology is associated with new toxicities that have not been common until now, which must be taken into account in the differential diagnosis of each clinical situation.
Clinical Case
A 55-year-old male patient had a diagnosis of squamous cell carcinoma of the lung, located in the left upper lobe, mediastinum and with brain metastases at baseline. He started treatment with chemotherapy and immunotherapy, with good clinical tolerance and an objective response at pulmonary level. One week after receiving the third cycle of treatment, he presented with a severe acute event at the Emergency Department.
The patient came to the hospital urgently for increased shortness of breath at rest, with central thoracic pain, and reported that he had felt feverish. He had been progressively reducing the dose of steroids he was taking at home, as an adjuvant to maintain his appetite and general condition.
In the emergency department, the patient was conscious, oriented, with shortness of breath and a feeling of severe illness. No fever was observed, but oliguria and hypotension were observed, alternating with high blood pressure, with an oxygen saturation of 97%, breathing oxygen. The blood count was normal (Hb:12), with moderate leukocytosis, prothrombin time of 61%, impaired renal function with creatinine of 1.6, uremia 125, glomerular filtration rate of 37 mL/min. Ions were normal, and there was a very significant increase in transaminases, more than five times their normal value (GOT 1010, GPT 1585), with minimally elevated total bilirubin values (1.6). The troponin value was normal. PCR 95. Venous blood gases: pH: 7.3; HCO3: 15.
The patient’s tendency to oliguria remained unchanged.
Clinical evolution. Decision making
First therapeutic diagnostic decision
As the patient had received oncological treatment with immunotherapy, in addition to chemotherapy, hepatic and renal toxicity due to immunotherapy was considered, and treatment with high-dose methylprednisolone was initiated.
Rationale
Immunotherapy toxicity can have a severe effect on several organs. Therefore, the decision to start high-dose steroids is correct, because it may save the patient. However, there are unusual findings in this type of toxicity, such as hypotension and oliguria.
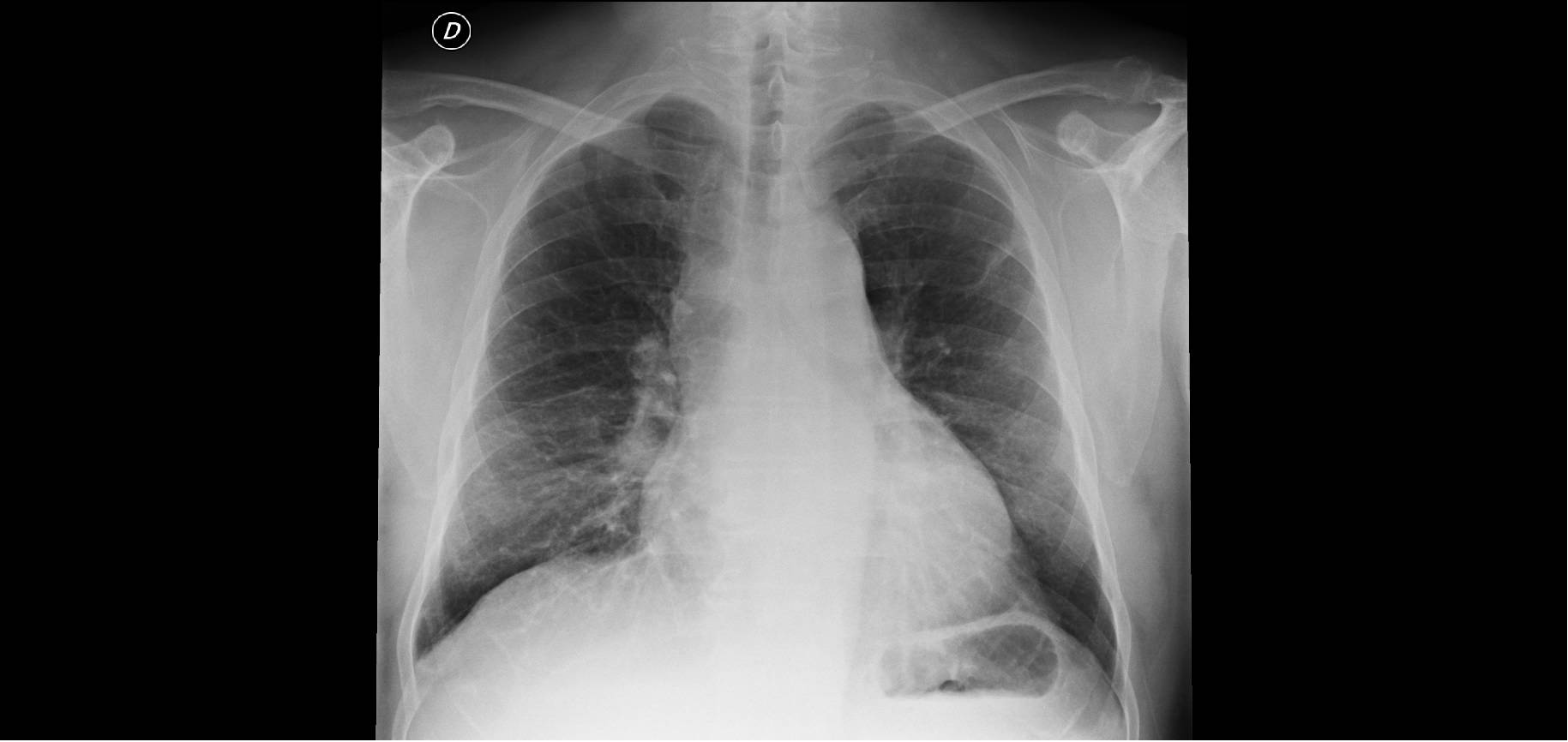
A chest X-ray on, admission is shown below:
Second diagnostic and therapeutic decision
Due to the acute presentation of the symptoms, with hypotension and oliguria, and elevated CRP, the possibility of a septic condition was assessed, and treatment with broad-spectrum antibiotics was started. Bilirubin elevation and alteration of transaminases may be present in sepsis due to hepatic hypoperfusion. The possibility of viral hepatitis was also assessed, because the anti-core and anti-HbS antigen (HBsAg) were positive, but the viral load was negative.
Rationale
A septic episode begins acutely, and in addition to non-specific signs such as restlessness, it is often, but not always, accompanied by hypotension and oliguria, ominous signs for the patient’s life. Liver abnormalities may also be present in septicaemia. Although elevated PCR may be indicative in this regard, elevated PCR in a patient with a neoplasm is of relative value in predicting infection. On the other hand, clinical response is usually relatively rapid after early initiation of antibiotics, but this was not the case in this patient.
Clinical Evolution
Twenty-four hours after the emergency department visit, the patient began to present more respiratory distress, a worse general condition, and was still oliguric and hypotensive. Pulmonary auscultation showed wet crackles in both bases, while cardiac tones were hardly audible.The hepatic border could be felt in the abdomen and caused some discomfort. The patient had to be transferred to the intensive care unit (ICU) due to hemodynamic instability.
The thoracic X–ray taken during the transfer to the ICU is shown below.

Question
What would be the relationship between low cardiac output, impaired liver function and renal failure?
Guidelines for the diagnosis of the situation
We have two allies to try to find an answer to the patient’s problem, Anatomy and Pathophysiology. In terms of pathophysiology, the first problem appears to be a ‘failure’ of the cardiac pump, resulting in hypotension and oliguria due to a lack of blood flow to the kidney, once it has been ruled out that the patient was not anaemic. As for the hepatic analytical alterations, this could also be related to a lack of perfusion, but this mechanism does not explain the painful hepatomegaly detected during the physical examination.
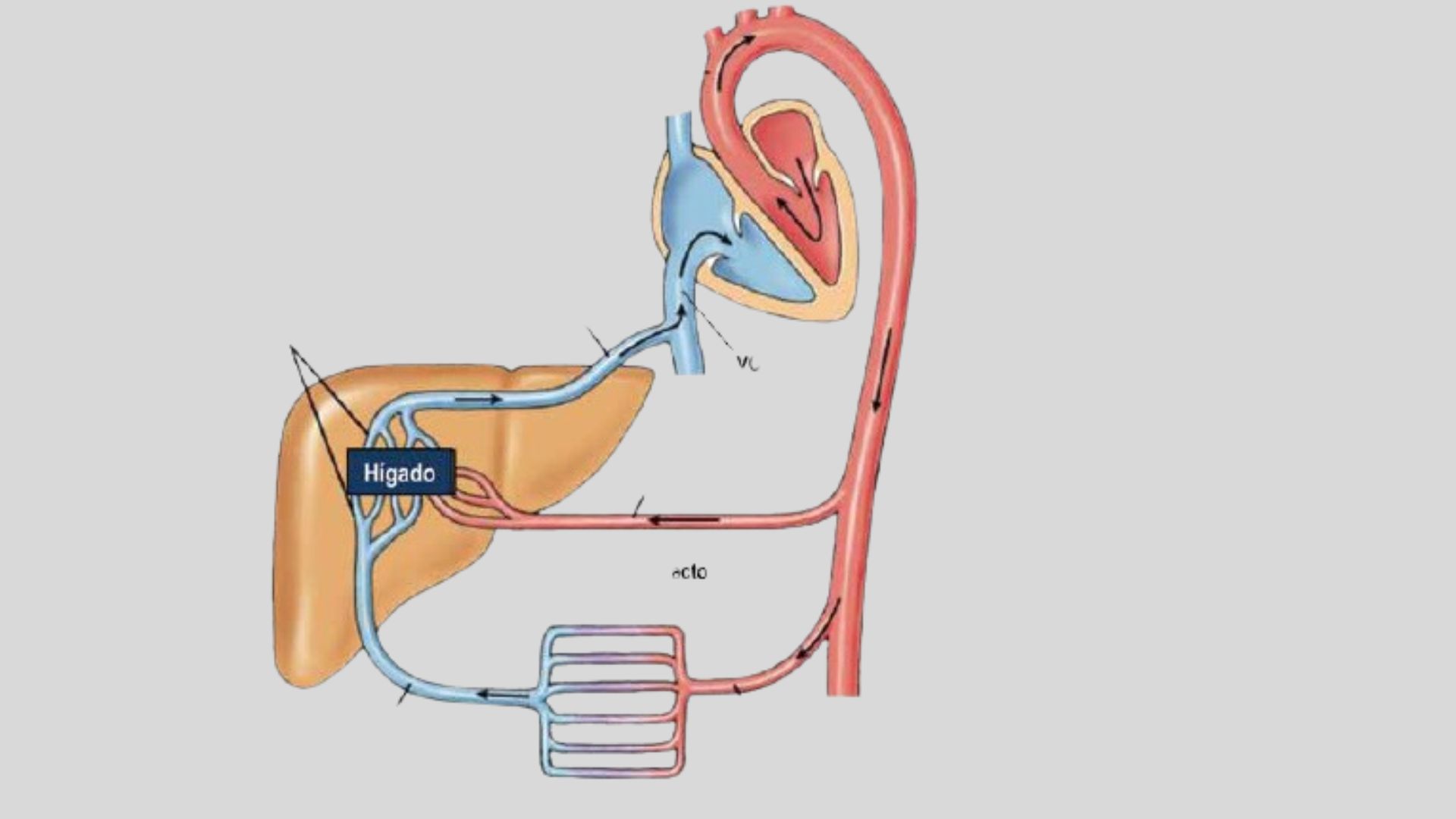
If we think from an anatomical point of view, the question would be whether there is any connection between the cardiac function and the liver, which would explain the analytical and morphological liver alterations.
A schematic anatomical image is shown below, which may help to explain the findings in this patient and to reach a diagnosis.
Solution. Final diagnosis
The patient underwent an echocardiogram which showed a heart with normal left ventricular contractility, no valvular heart disease, but there was severe circumferential pericardial effusion, with systolic collapse of the right atrium, systolic collapse of the right ventricle, and a dilated inferior vena cava without inspiratory collapse. This situation was responsible for hypotension, oliguria due to low output, and hepatomegaly and hepatic analytical alterations, due to retrograde congestion from the right atrium to the inferior vena cava and liver.
Comment
In addition to knowledge of the different clinical entities, the process of clinical reasoning has a strong basis in Anatomy and Physiopathology, as we have shown in this clinical case, in which an anatomical structure such as the inferior vena cava can help to explain the patient’s data.
Author: Lorenzo Alonso Carrión
FORO OSLER


