Clinical reasoning: When the symptoms of the patient fit the Data Base

Objective
When a disease is not common and their signs and symptoms can be shared with other entities, a particular detail can give an important clue to reach the diagnosis. There is a lot of clinical information today for every clinical picture and clinical database can select one of these characteristics.
In this clinical case we want to highlight the importance of a complete knowledge of particularities in the clinical presentation of a process, some uncommon but well defined presentation that can help us to save the life of a patient, and also we want to enhance the key role of the laboratory medicine in the diagnosis of a disease.
Clinical case
A-35-year-old Peruvian man without any previous disease started with intermittent nausea and vomiting, ataxia and dizziness, maintaining these symptoms for a month, consulting at least twice to a hospital. After this time, the patient started with less strength in the left arm, with diplopia, so he went to the hospital.
During the physical examination he was alert and orientated with a normal speech and a normal general examination.There was no fever at the moment of the examination. The neurological examination showed an impossibility to walk, with a dismetry predominantly in the left hemibody. No stiff neck was present. There was an impairment of the ocular convergency, without deficit in any other cranial nerves.
Blood test, biochemistry, renal function and coagulation were normal. Antigen for virus SARS-CoV-2 was also negative. A thoracic X-ray was normal.
Because the patient referred occasional fever at home , a blood culture was obtained.
Patient Illness Script
“This is the case of a previous healthy young man that started in an acute form with fever, vomiting, and gait coordination problems, lasting for almost a month, with cranial nerve palsies in the evolution, almost a month later. I would think in a intracranial hypertensive syndrome (nausea and vomiting), with a cerebellar problem (gait disturbances), possibly associated with an unknown infectious etiology”
What is your diagnosis?
Maybe you recognize a pattern here or maybe not. A pertinent question would be: Is there any infectious disease, starting in an acute presentation, with a predominant tendency to a cerebellar involvement in a healthy man? This is a difficult question to answer even for a neurologist.
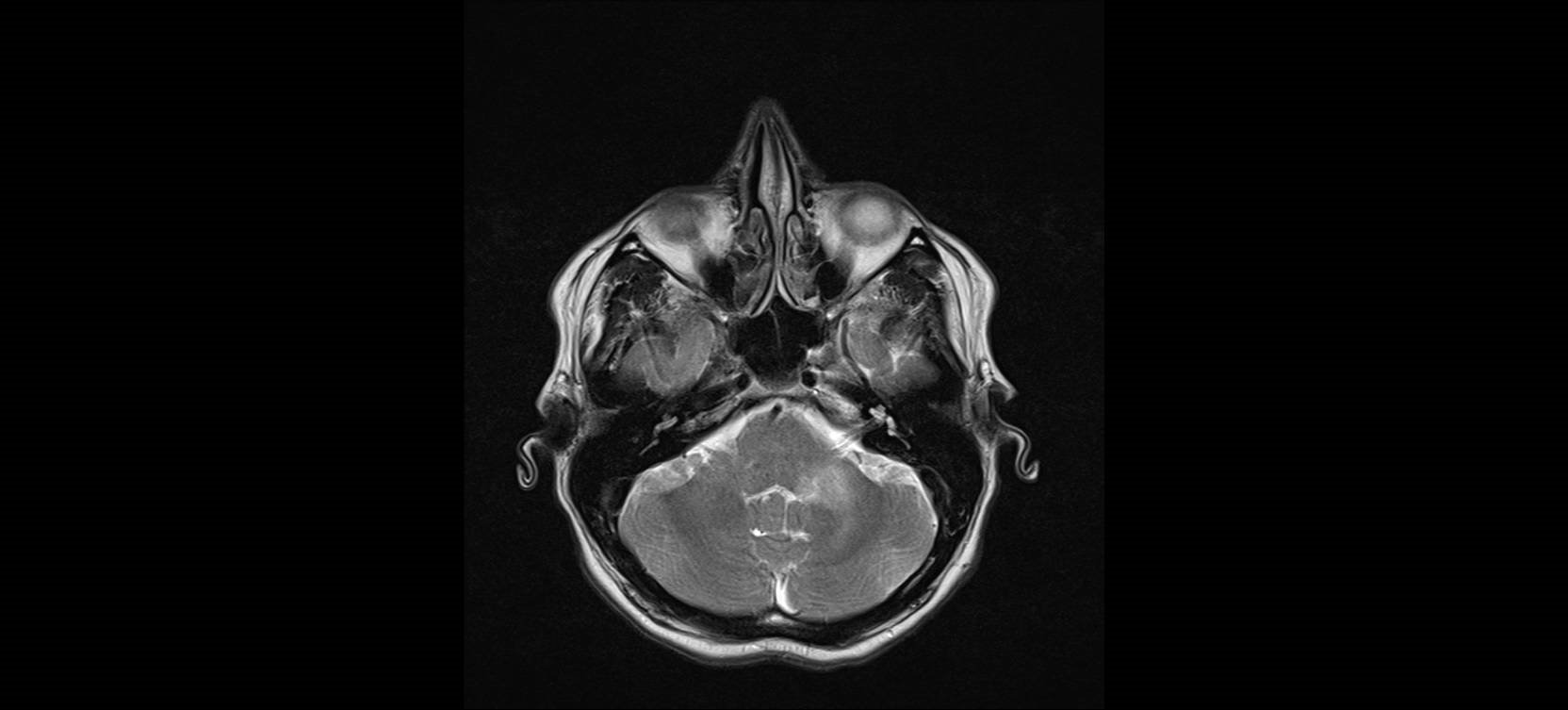
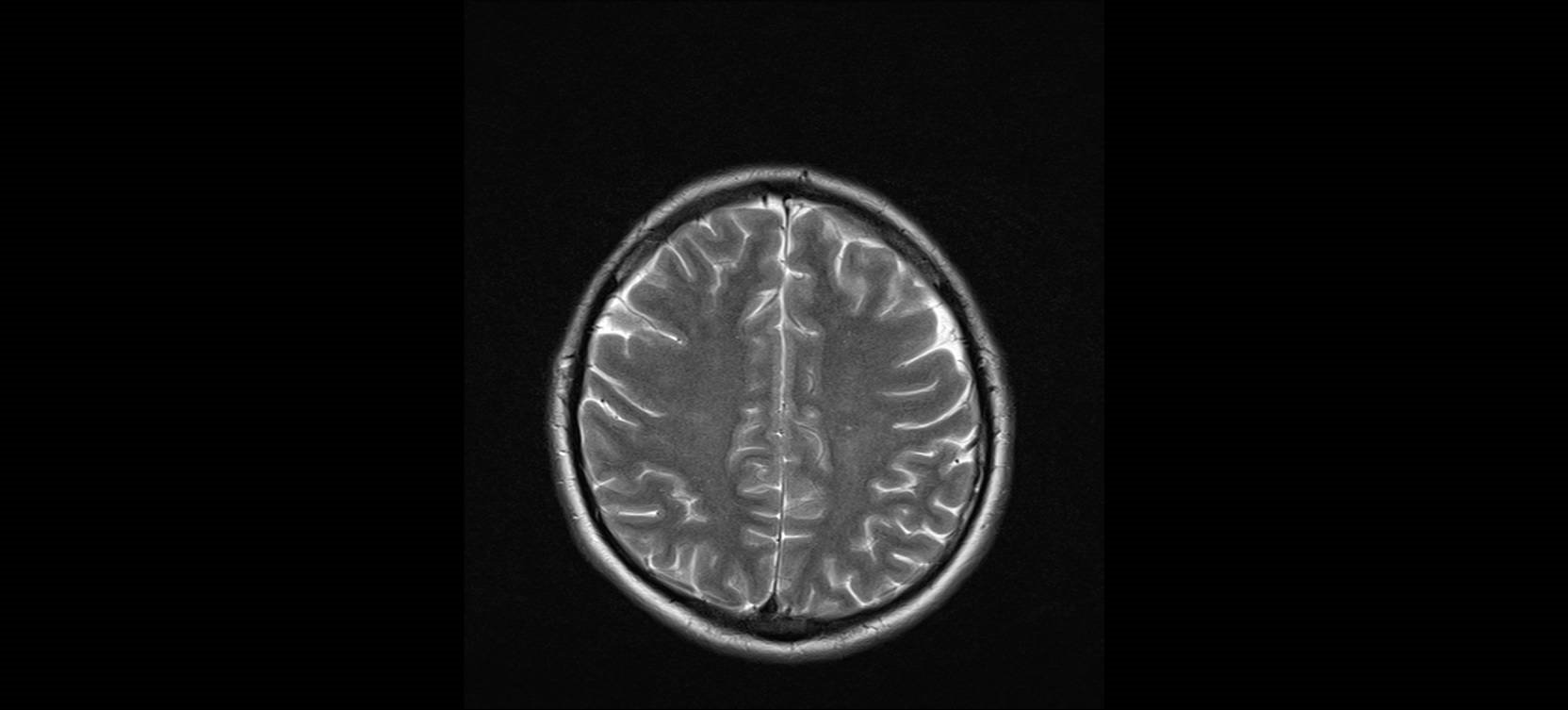
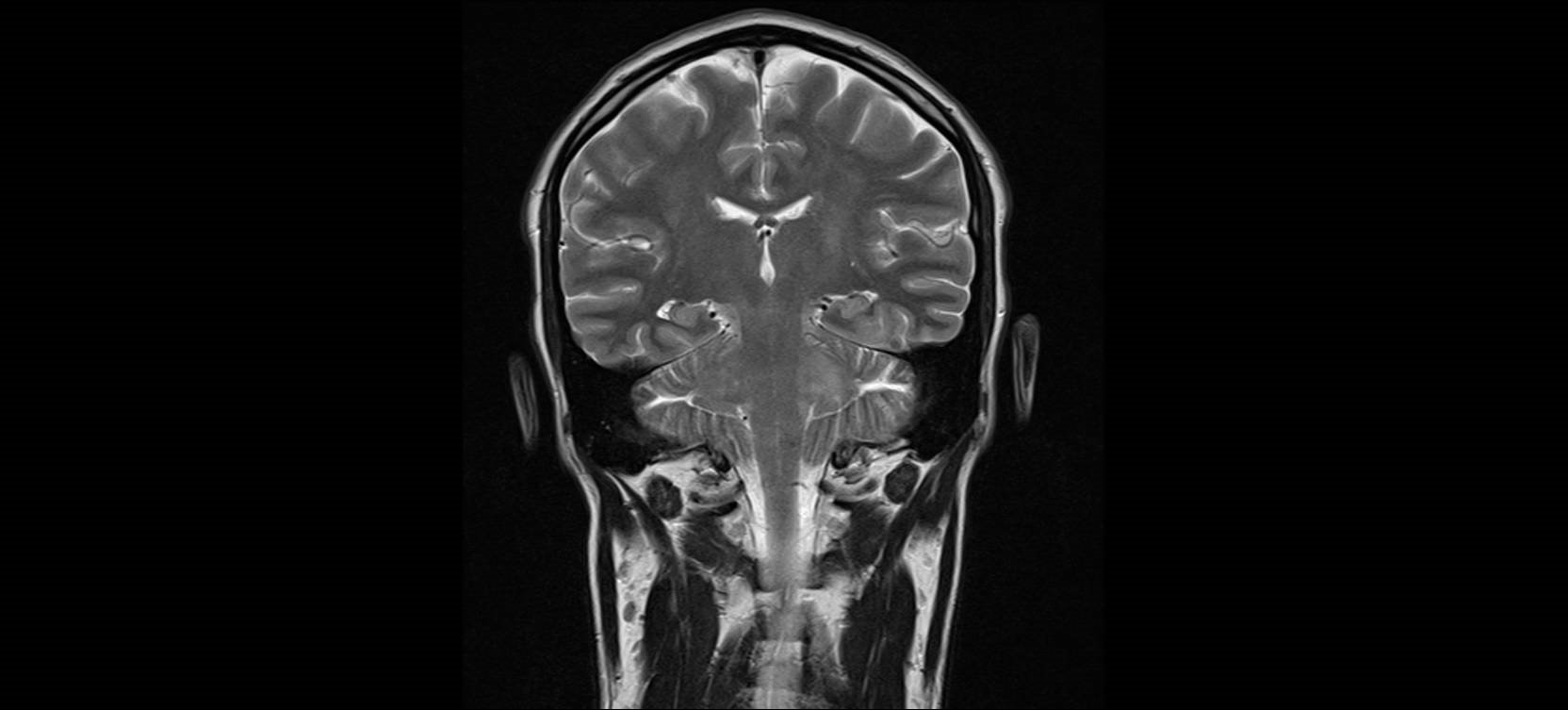
To help with your reasoning, we will expose here some images from the patient
What do you think was the test for a definitive diagnosis?
You can know the answer here
Author: Dr. Lorenzo Alonso Carrión
FORO OSLER


