
Resist and not give up: the key to fighting premature closure
A 62-year-old woman went to the Emergency Department(ED) with a colicky pain located in the abdominal right upper quadrant with irradiation to periumbilical area, starting two days before, with
nausea and vomiting. No fever was present. She has no previous disease or a surgical intervention. She had six children.
Physical exam: the right upper abdominal area was tender under pressure, but no liver enlargement was detected. The rest of the physical exam was normal.
First Diagnostic Hypothesis: The young doctor established “gallbladder stones” as his first diagnostic hypothesis, but the ultrasound didn´t show that. Then, the doctor decided to repeat the physical exam and, at this time, he paid attention to a lack of bowel sounds, driving his reasoning to the bowel as the origin of the symptoms. He asked for a plain abdominal X-Ray.
Diagnostic Image:
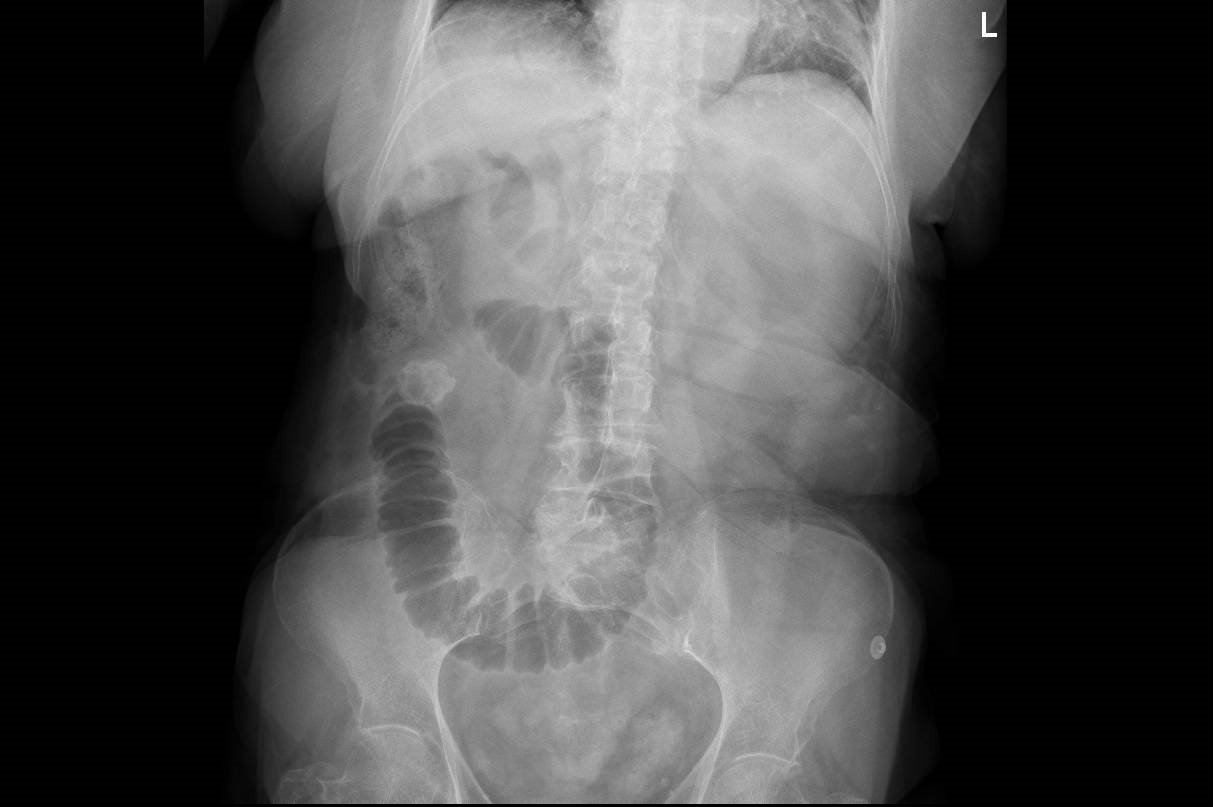
Clinical evolution: The finding focused the attention in the small bowel, but the cause of the problem was not clear yet. At that moment the patient was without pain under the effect of a strong painkiller and the possibility of a final diagnosis such as “biliar colic” was very high. But, then the intuition of the doctor puts him in the path to look for more answers. Asking for a CT scanning is not an easy task in every ED around the world, but this time with the help of a surgeon, the radiologist accepted to do it.
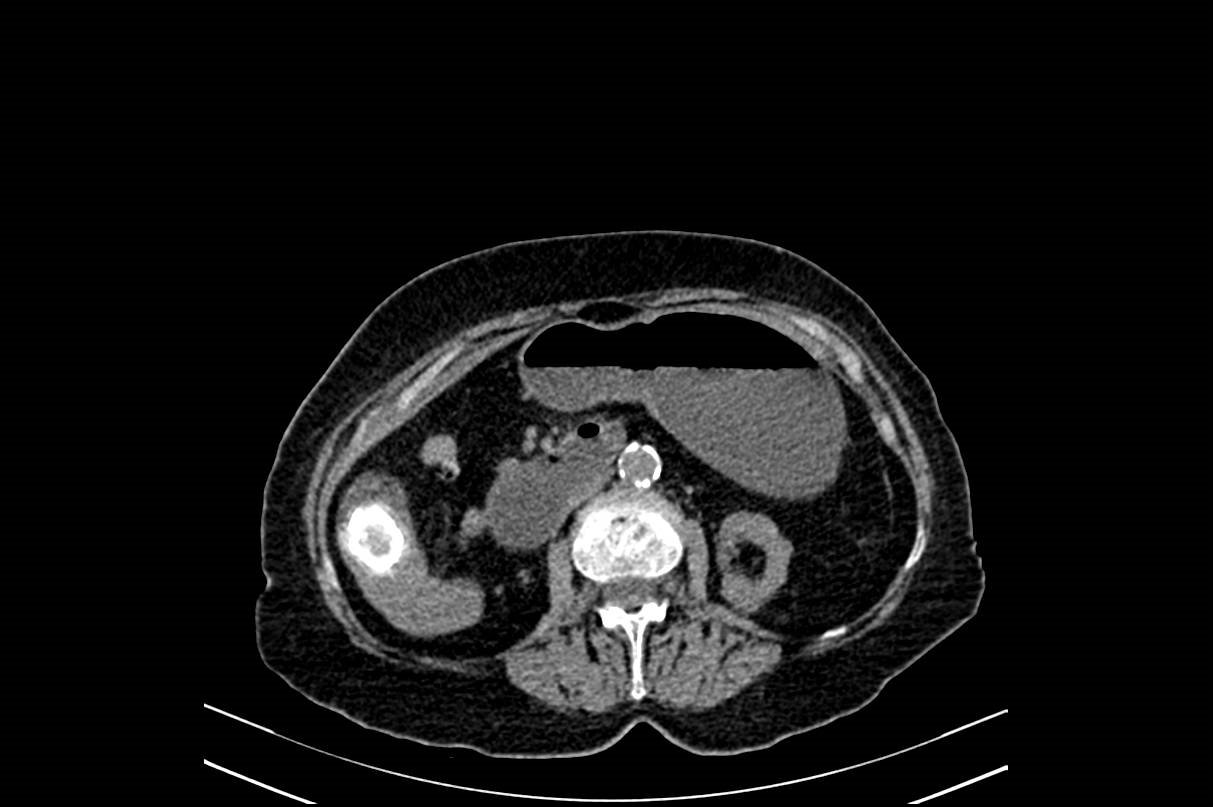
Final Diagnosis: Gallstone Ileus
Comments: Premature closure is a cognitive bias that can be present when the clinical problem is not common or the presentation is unusual. In this clinical case only the persistence of the doctor looking for more information allowed to reach to a correct diagnosis.
Author: Lorenzo Alonso


