Spinal cord compression: when a wider differential diagnosis is essential
- Important Notice: The image showed here has the patient´s consent. No real data for identification are provided.
Clinical case
A 54-years-old-man, with a previous diagnosis of benign prostatic hyperplasia, went to the Emergency Department (ED) because of fever in the last ten days. He also referred to be unable for walking in the last two days, without strength on their legs.He was born in Kenia, but he had been living in the last ten years in Spain, travelling occasionally to Africa.
Clinical evolution
He was alert and conscious during the physical examination. The only abnormal finding was a paralysis on both legs, without strength to move them up while standing on the bed. There was a lack of perception of a medium dorsal level.
Six hours after the visit to the ED a blood culture was obtained due to the presence of high fever and chills. and the doctor decided to start with antibiotics.
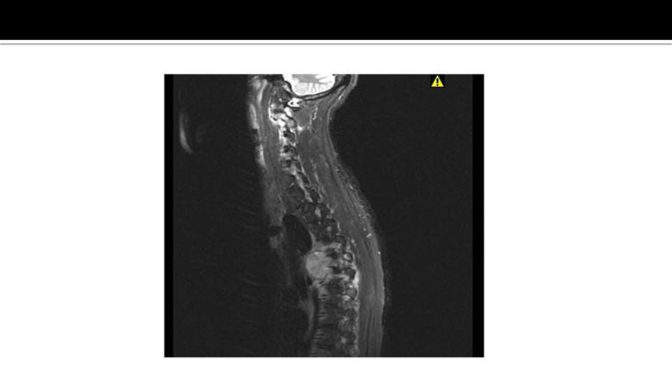
In the next picture we show the CT scan of the patient:

Clinical reasoning
Initially was clear that the patient had an acute spinal cord compression with a motor and sensitive level. He started treatment with corticoids and the doctor asked for a consultation to the Radiotherapy Service.
Twenty-four hours later the patient started to feel better, without fever and he was able to move their legs. This situation was a surprise to the doctors who saw the patient at the first encounter.
The definitive diagnosis was obtained after a biopsy taken from the spinal lump, under radiological supervision.
Question
After reading the clinical summary and looking to the CT, what do you think is the most accurate diagnosis?
- Haemorrhage
- Infection
- Neoplasm
- Neurofibroma
If you want to know the answer and the Analysis of the case click here


