
Myocardial infarction in women: a cause of diagnostic delay
Myocardial infarction in women
Women with a coronary syndrome can have atypical symptoms
The coronary syndrome in a woman can start with atypical symtoms in comparison to a man. A pleuritic pain, a burning sensation, as well as dyspnea of unusual characteristics or pain in the upper back or in the epigastric area.
Sometimes the symptoms are associated with flu, dizziness, generalized feeling of fear / anxiety, weakness generalized, indigestion, or palpitation.

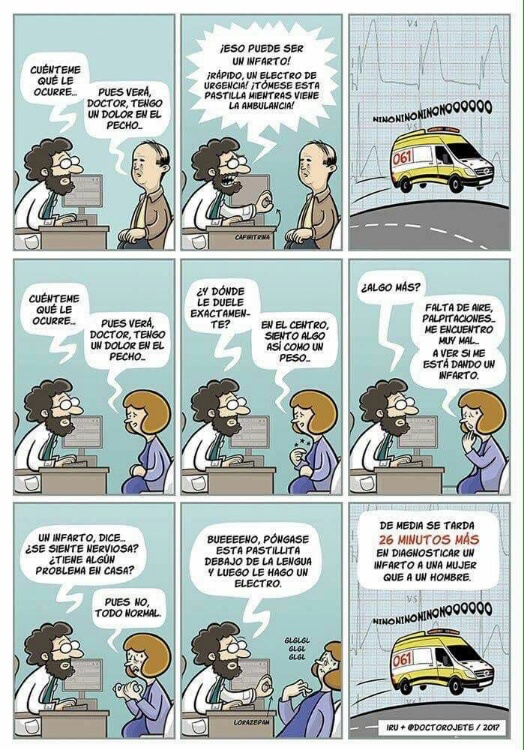
Coronary syndrome in women: a cause of diagnostic delay
Moreover, a woman does not recognize her symptoms as cardiac in origin, and this is usually a common cause for a delay in her diagnosis. In addition, by not recognizing the symptoms as serious, she puts family or housekeeping in the first place, before going to the doctor. Once she decides to go to the emergency department, the time until an electrocardiogram is performed, if it is done, is usually longer than in the case of the male.
Physiopathology is different in women
The female pattern of ischemic heart disease is different from the usual in a male. In the WISE study it was observed that more than 50% of middle-aged women with symptoms of chest pain, this is related to vascular dysfunction in the epicardial and microvascular vessels and not to an obstructive cause of ischemic heart disease. The coronary microcirculation consists of a network of small arteries and pre-arterial arterioles that make up approximately 90% of the coronary circulation. Diagnosing alterations in this vascular network remains a challenge. Clinical control of diabetes and hypertension are important factors also in women. Fortunately, with the passage of time we are starting to know more risk factors in women, such as the ones recently included in the guidelines on prevention of cardiovascular diseases of the 2016 European Society of Cardiology such as, for instance, a previous history of preeclampsia or HELLP syndrome, a clinical situation that was found to be one of the strongest risk factors in women.
Although the general pattern of coronary atherosclerosis is more diffuse and less obstructive in women, the clinical prognosis is not good. This may be because women tend to have coronary heart disease approximately 10 years later than men, so they tend to have more comorbidities (kidney disease, osteoarticular, anemia). Also, before menopause, women are partially protected by estrogens, but after the menopause, there is an increase in cholesterol and blood pressure levels.
Psychosocial factors also come into play. Depression increases the risk of suffering cardiovascular disease. Likewise, severe stress is also considered a trigger for cardiovascular disease in women. An extreme example is Tako-Tsubo cardiomyopathy, or apical ballooning syndrome, which is an acute coronary syndrome that occurs in women predominantly older than 60 years after an episode of severe emotional stress.
How to improve the detection of a coronary syndrome in a woman?Some advices are exposed:
1) Perform an electrocardiogram before any clinical suspicion in women even if they do not show the typical symptomatology of chest pain of ischemic characteristic 2) The population must be educated in the early recognition of the specific symptomatology associated with sex (The American Heart Association has made a decalogue with the priorities to improve outcomes in women with Acute Myocardial Infarction).
Therefore, as always in Medicine, we must pay attention to the context, in this case being aware that the clinical picture of acute coronary syndrome in women, although it may occur in the same way as in men, may appear with atypical signs and symptoms, that could be associated with non-important problems such as anxiety and depression. To avoid errors of diagnosis and reducing mortality, we must know this fact, and then we will improve the diagnosis and therapeutic decisions in this group of patients.


