
Clinical reasoning in practice: a change in the voice
Clinical reasoning in practice: a change in the voice

Clinical summary
A 57-years-old man with a diagnosis of non-small cell lung cancer with a mass located in the posterior area of the left lung. He was transferred to the hospital because he felt suddenly a sensation ofconscious loss, without thoracic pain or dyspnea. He recovered from this situation and an MNR showed an image compatible with a cerebral cortical infarction.
Five days later, during the stay at the hospital, he acutely started with a left thoracic pain with more dyspnea and irradiation to the left arm. The doctor on call that night examined the patient and she asked for an EKG and cardiac enzymes, but they were normal. She prescribed an analgesic and oxygen and the patient felt better.
Next morning, when the attending doctor visited the patient, he noticed a change in his voice, like more nasal. He suddenly remembered another similar less than a month ago, and this sign, together with a pulmonary auscultation, was key to a correct diagnosis .
#Question 1
Now in this patient with a lung cancer, acute thoracic pain and a change on his voice, Can you suggest a diagnosis?
#Question 2
Do you know the mechanism involved to explain the change in his voice?
If you want to know the answer click here
Final Diagnosis
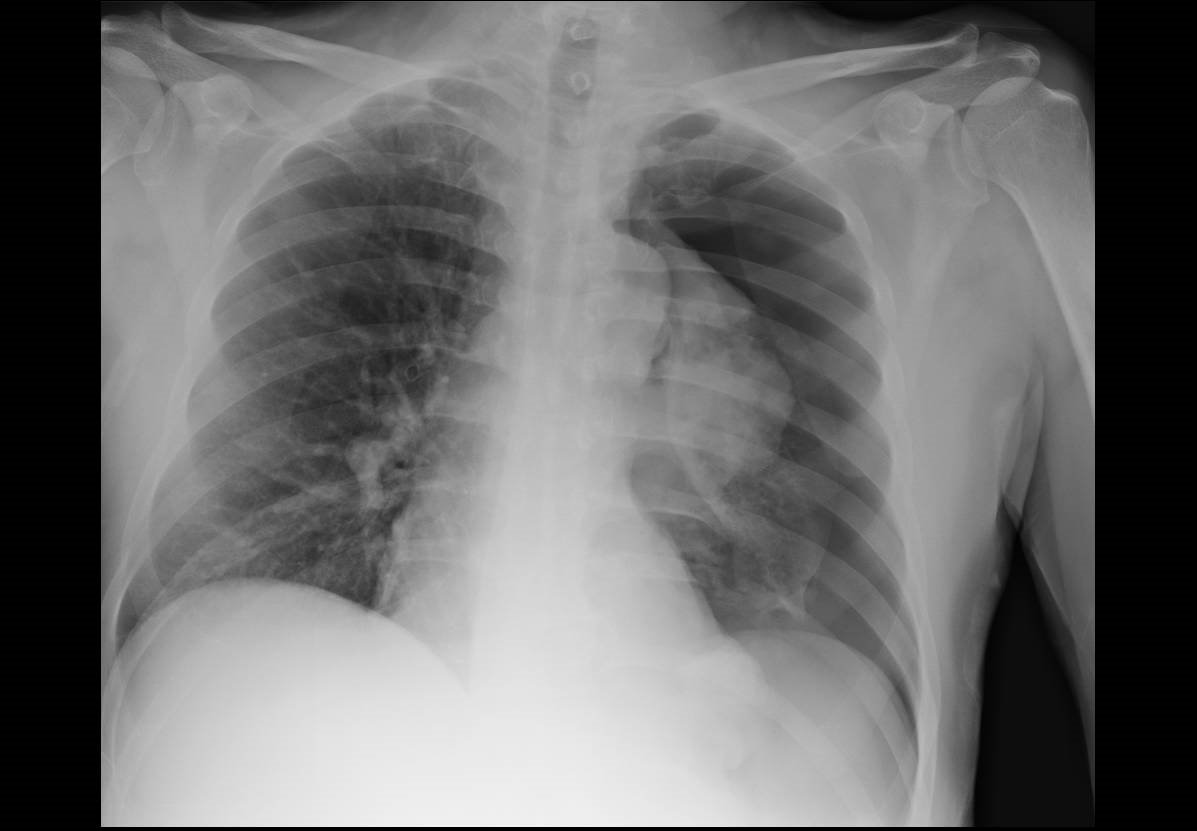
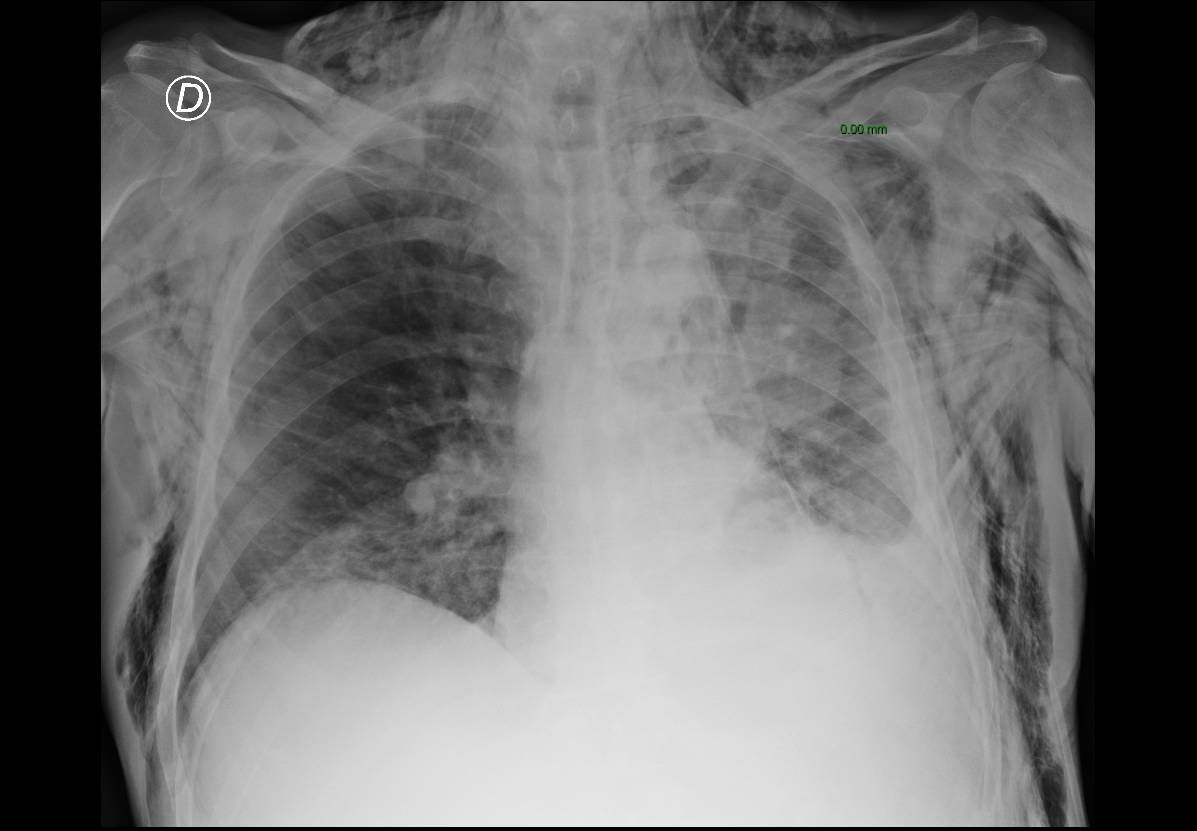
Left pneumothorax due to infiltration of the visceral pleura from the tumor. The change in the tone of the voice is associated with the increase of pressure over the recurrent nerve.
In the next images we can see the pneumothorax, the tumor and the subcutaneous emphysema associated.
Clinical reasoning
The first doctor followed her illness script for a myocardial infarction, shaped with an acute thoracic pain with irradiation to the left arm, however, after a normal EKG and normal cardiac enzymes, the probability of this diagnosis was clearly reduced. Moreover, a wider differential diagnosis would have been very useful.
Another important factor to consider is the reduction in the alert level in an emergency situation after several hours of work and during the night time.
Definitely, a safe and practical attitude is always to be methodical about physical examination. In this case the pulmonary auscultation was clearly abnormal.
Usually, the availability heuristic is shown as a bias for a wrong decision, where a recent experience or an emotional one, can blur the correct election. However, in this case, the past experience not long ago with a similar patient, help the doctor to achieve the correct diagnosis.
Bibliography
Méndez Garrido S, Ocete Pérez RF. Causes and imaging manifestations of paralysis of the recurrent laryngeal nerve. Radiologia. 2016 May-Jun;58(3):225-34. doi: 10.1016/j.rx.2016.02.008. Epub 2016 Apr 8. English, Spanish
Author: Lorenzo Alonso. Foro Osler


