People with disabilities: a group prone to a diagnostic delay
Introduction
Biases associated with specific populations, for example with female gender or particular ethnic groups, are well known and often lead to a diagnostic delay.
Objective
To highlight the importance of assessing people with special circumstances, when attempting to make a diagnosis.
Clinical case
A 24-year-old male patient presented with motor disturbances since birth associated with hypoxemia during delivery. He was also diagnosed with hebephrenic schizophrenia and was taking specific medication for it, together with other sedatives.
Two months before the current diagnosis, the patient began to feel tired and with some decrease in appetite. He went into primary care at least three times, but his symptoms were always related to side effects of antipsychotics.
There were difficulties with the anamnesis but not with the physical examination, which was generally considered normal, although the inguinal region and testes were not examined.
Clinical course
The patient continued with asthenia, weight loss and hyporexia, starting with diffuse abdominal pain, without nausea or vomiting. A CT scan of the abdomen showed the presence of retroperitoneal lymphadenopaties.
A new complete and directed examination detected the presence of a mass in the left testicle. In the following days, a left inguinal orchiectomy was performed, and the pathology report was informed as “malignant tumour, seminoma type”.
Analysis of the case
Definition of error: a diagnostic delay (it took at least two months to reach a diagnosis, after the symptoms started).
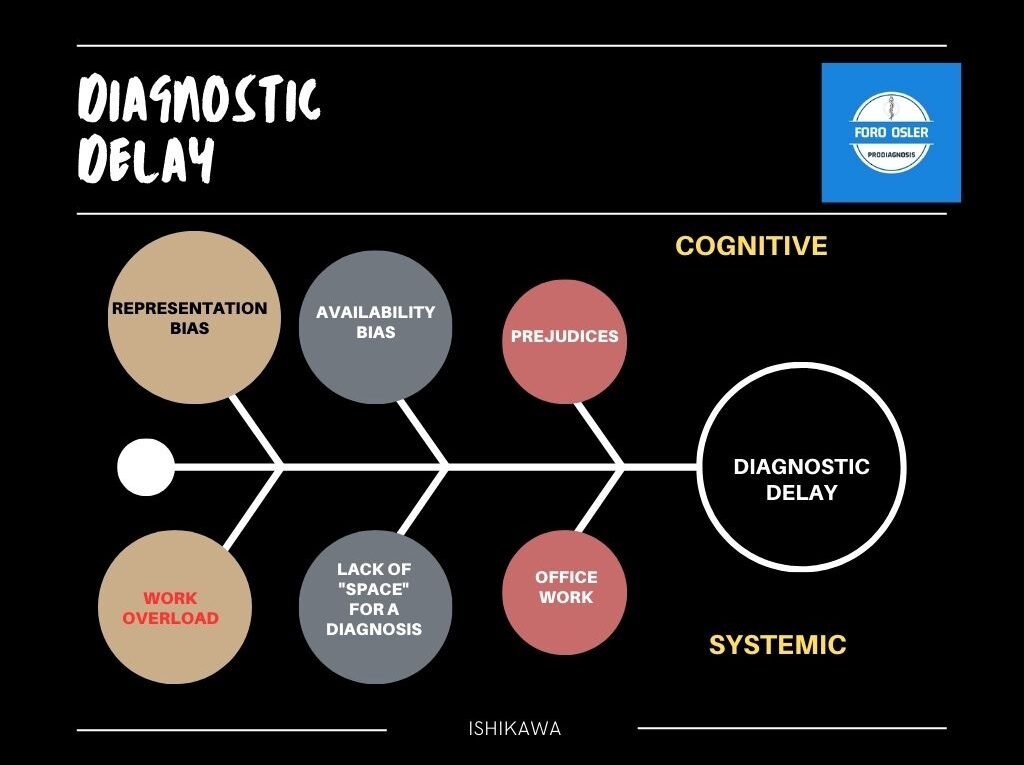
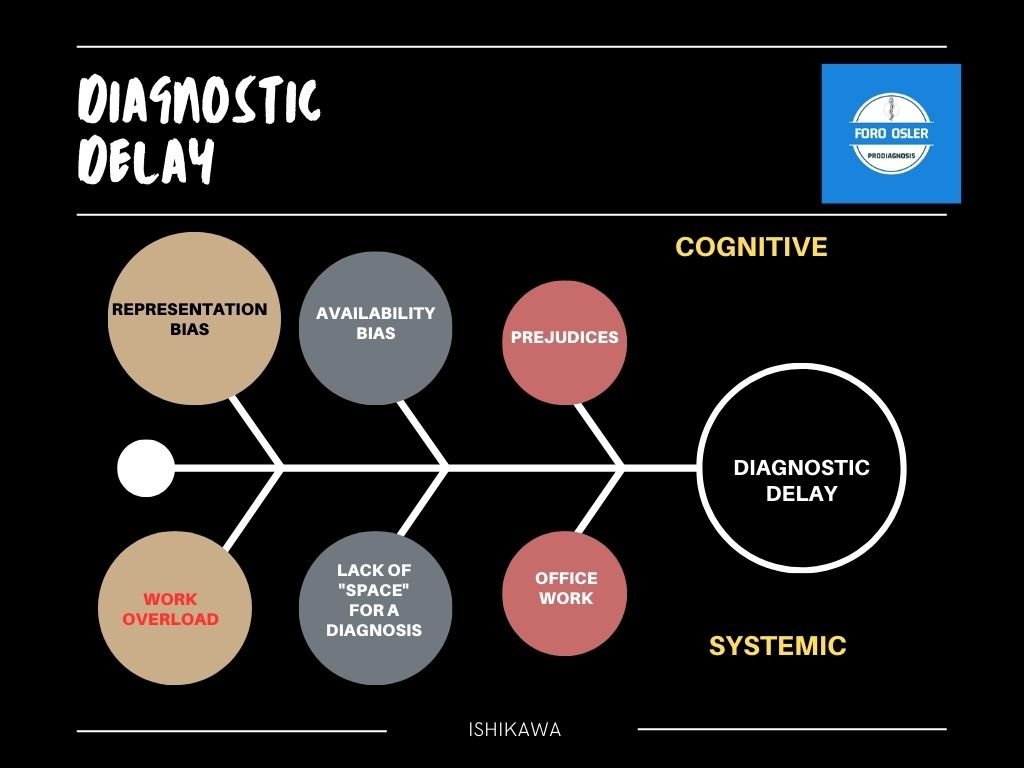
Factors involved
Cognitive biases: we can consider that there was a representation bias, i.e. attributing symptoms to the patterns we have in the brain, or even availability bias, attributing symptoms to what comes most easily or quickly to mind, based on previous experience.
Systemic factors
Generally, primary care consultations are often overloaded and there is no specific place and time to perform a thorough and complete physical examination.
An important factor is that the opinion of the relatives of patients who are unable to express themselves may not be fully taken into account.
Improvement measures
– When seeing a patient for the first time, the physician should be as objective as possible in his or her care, without preconceived ideas.
– Certain people or populations with their own characteristics may favour the appearance of cognitive biases in the health professional, sometimes due to “mental exhaustion” that makes them look for an easy way out, shortening the clinical reasoning process.
Author: Dr. Lorenzo Alonso Carrión. FORO OSLER


