A quick communication about a first impression of the patient is a good practice

A quick communication about a first impression of the patient is a good practice
Diagnosis is quite often an episode of anxiety
When a person has a health problem , the first contact with a health facility could be your personal doctor , your general practitioner (common in socialized health services), or the EmergencyDepartment (ED). These two last facilities are usually overcrowded and the idea about going there is frightening and disturbing, and it is not a less important issue the time that families spend waiting for some news. At the end your problem will resolve, but , can we think in a magic bullet necessary to improve this momentum?.
Good communication and a quick idea about the problem
One important thing for the patient, the family and the system is to reduce the amount of time waiting for an answer. Of course, it is not easy in a crowded, busy and risky environment to give an explanation to a patient, but this should be also a doctor´s duty.
Nowadays, emergency department interns and doctors work as if they were in a military environment or in an ensemble line, classifying patients, prescribing them a “standard” treatment based on signs and symptoms and waiting for the result of blood and other tests,, but if you look to the clinical judgment paragraph possibly you will see a blank space. Maybe this situation is not common in your work environment , then you are lucky, but it is common in many places around the world. The first impression, the first clinical judgment, is the product of the experience and the clinical evaluation, and must be expressed even before the result of the arrival of the tests.
The first idea, the first prognosis: the sooner the better
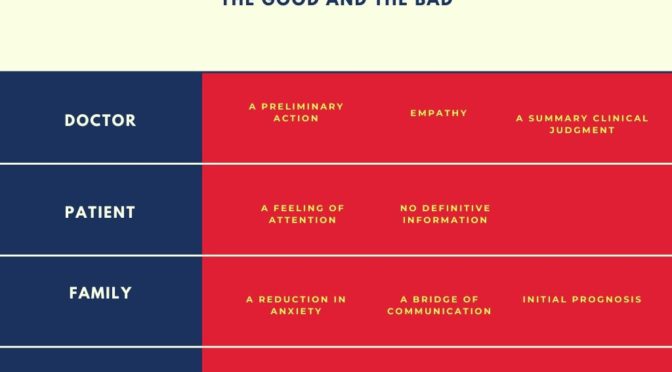
General public, even the media, have the idea about medicine as a question of quantity, every problem will be fixed if you increase the number of doctors and nurses, the number of CT machines, etc, but the truth is more complicated because, at the end, the real limit is inside the physician´s mind. When a doctor is attending a patient in the ED he or she needs to have an idea about the patient´s problem, it could be a syndrome or just a “working diagnosis”, to start with a therapeutic action, but usually this idea is kept inside until the results of a blood test or an image are evaluated. There is a logic “risk aversion” to communicate a preliminary information to the family or the patient, and even is a way to observe the patient in more detail, with more time. But, there must be something in the middle, before the arrival of the whole results of the test, what is in my opinion good for the patient, the family, and for the system and this is the proposition to communicate this preliminary diagnosis or idea about the patient, with the consequence of less anxiety and more trust between the family and the doctor.
This first idea must be based on a syndromic approach, more a description of the problem, and the possible clinical evolución. The information must be communicated to a member or members with a direct relationship with the patient, and it is also important a proper place with enough confidentiality.
Author: Lorenzo Alonso, MD.


