A Clinical Reasoning Exercise: Dysmetria, Nausea, Vomiting, Trouble to Speak

A Clinical Reasoning Exercise: Dysmetria, Nausea, Vomiting, Trouble to Speak
Clinical Case
A-52-year-old man with a previous diagnosis of an esophageal carcinoma , went to the hospital with nausea, vomiting and constipation. He had no fever or abdominal pain. The physical examination showed no bowel movements. The neurologic examination showed a gait disturbance, dysmetria and difficulty speaking properly. A nasogastric tube was inserted and a big amount of liquid was extracted from the stomach.
Comment
The symptoms of nausea, vomiting and constipation could orientate the first diagnosis to an ileus associated with an abdominal recurrence of the tumor. There are also neurologic symptoms that need to be integrated into the clinical diagnosis of the patient. These symptoms also could be associated with the spreading of the tumor to the Central Nervous System (CNS).
Clinical Evolution
An abdominal CT scan showed a left adrenal gland metastasis , but no infiltration of the Bowel , without signs of intestinal obstruction. The patient was able to eat some soft food and liquid. A CNS scan without contrast was considered as normal. The patient started with agitation and in a new neurological evaluation was detected a clear bilateral nistagmus. He could move his four extremities without any problem.
Comment
The possibility of an abdominal recurrence was not discharged, but now the clinical reasoning process of the doctor was orientated to the CNS.
It is usually normal to associate some symptoms, such as nausea and vomiting, with the digestive system, even more so when the diagnosis was of a digestive neoplasm. But, we must remember, that the nervous system controls both the motor and the autonomous sides and that an intracranial hypertension syndrome causes headache, nausea and vomiting.
Clinical Evolution
The general condition of the patient suffered a deterioration, with altered mental status, a gait disturbance, dysmetria and more trouble to speak. The medical oncologist made a short differential between encephalitis, but no fever was measured, viral or bacterial meningitis, but there was no neck stiffness or meningeal carcinomatosis.
Comment
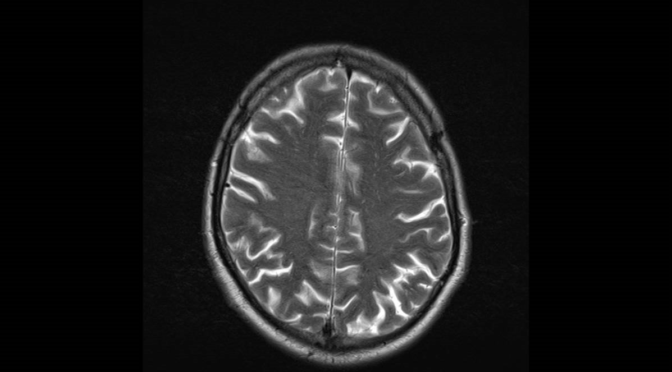
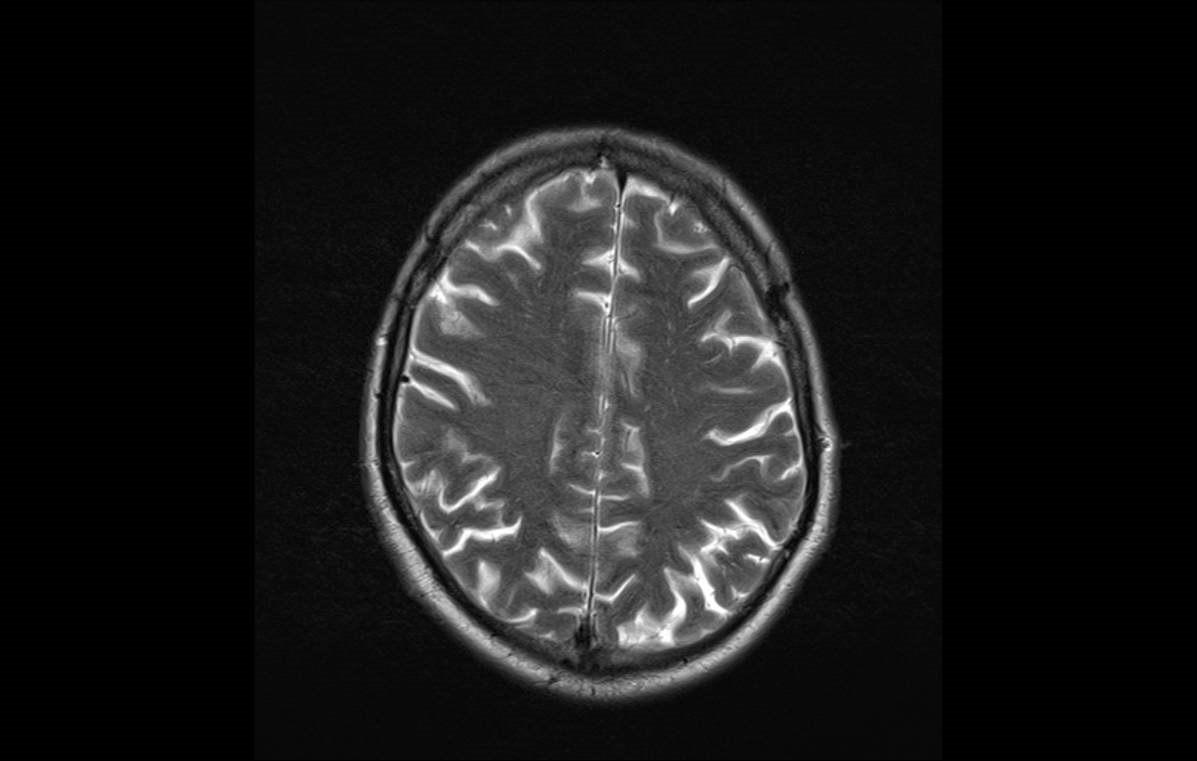
Meningeal carcinomatosis is a very well known diagnosis for a medical oncologist. Some tumors can disseminate to the CNS via cerebrospinal fluid. There are different types of symptoms, most of them related to cranial nerve involvement, cerebellar infiltration or intracranial hypertension. An MRI is the best diagnostic test for diagnosis, showing an increase in the brightness of the meninges. A lumbar puncture to extract cerebrospinal liquid for a cytologic study can be definitive, but it is usually positive in only one third of the cases. In this case the study of the cerebrospinal fluid showed the presence of tumor cells.

Final Diagnosis
- Meningeal carcinomatosis , cerebellar metastases and intracranial hypertension
Bibliography
Leptomeningeal metastasis from systemic cancer: review and
update on management. Nancy Wang, M.D.1, Mia S. Bertalan, B.A.1,2, Priscilla K. Brastianos, M.D. Cancer. 2018 January 01; 124(1): 21–35. doi:10.1002/cncr.30911
You can reach a review about meningeal carcinomatosis here
Author: Dr. Lorenzo Alonso
FORO OSLER


